





















Laryngomalacia is a common congenital condition that affects the larynx, the voice box, in infants. It is characterized by the abnormal softening and inward collapsing of the tissues of the larynx during breathing. This condition often becomes noticeable within the first few weeks of a baby’s life and can cause a variety of symptoms, ranging from mild to severe. In this article, we will unveil laryngomalacia by exploring its signs, causes, and implementing effective management strategies for this condition.
Understanding Laryngomalacia
Laryngomalacia is the most common cause of congenital stridor, a high-pitched sound heard during breathing. It occurs when the tissues of the larynx are floppy and collapse inward during inhalation. While the exact cause of laryngomalacia is unknown, it is believed to result from the immaturity of the laryngeal structures. Fortunately, laryngomalacia is a self-limiting condition that typically improves as the infant grows and the laryngeal tissues mature.
Signs and Symptoms of Laryngomalacia
1) Inspiratory Stridor
One of the hallmark signs of laryngomalacia is inspiratory stridor, a high-pitched, wheezing-like sound that occurs when the baby breathes in. This sound is most noticeable during periods of increased activity or agitation and often worsens when the baby lies on their back. Inspiratory stridor is caused by the partial obstruction of the larynx due to the collapsing tissues.
2) Retractions and Noisy Breathing
Laryngomalacia can also cause retractions, which are visible inward movements of the chest wall or the area just above the breastbone during breathing. These retractions occur as the baby exerts more effort to overcome the obstruction in the larynx. Additionally, noisy breathing, such as snoring or rattling sounds, may be present.

3) Feeding Difficulties
Some infants with laryngomalacia may experience feeding difficulties. The combination of increased effort required to breathe and swallow simultaneously can lead to poor coordination during feeding, resulting in frequent interruptions, coughing, choking, or difficulty gaining weight.

Causes and Risk Factors
1) Immature Laryngeal Structures
Laryngomalacia is thought to occur due to the immaturity of the laryngeal structures at birth. As the baby grows, the larynx usually develops and strengthens, resolving the symptoms.
2) Gastroesophageal Reflux (GERD)
Gastroesophageal reflux, a condition in which stomach acid flows back into the esophagus, can exacerbate the symptoms of laryngomalacia. The acid reflux irritates the already sensitive larynx, causing increased inflammation and tissue collapse.

3) Neurological Conditions
In rare cases, laryngomalacia may be associated with certain neurological conditions, such as Chiari malformation or cerebral palsy. These conditions can affect the coordination of the muscles involved in breathing and swallowing, contributing to laryngeal collapse.

Diagnosis and Evaluation
The diagnosis of laryngomalacia is primarily based on a physical examination and a thorough medical history. The healthcare provider will listen for the characteristic inspiratory stridor and observe any associated symptoms. In some cases, further evaluation may be recommended to rule out other underlying conditions or assess the severity of the laryngomalacia.
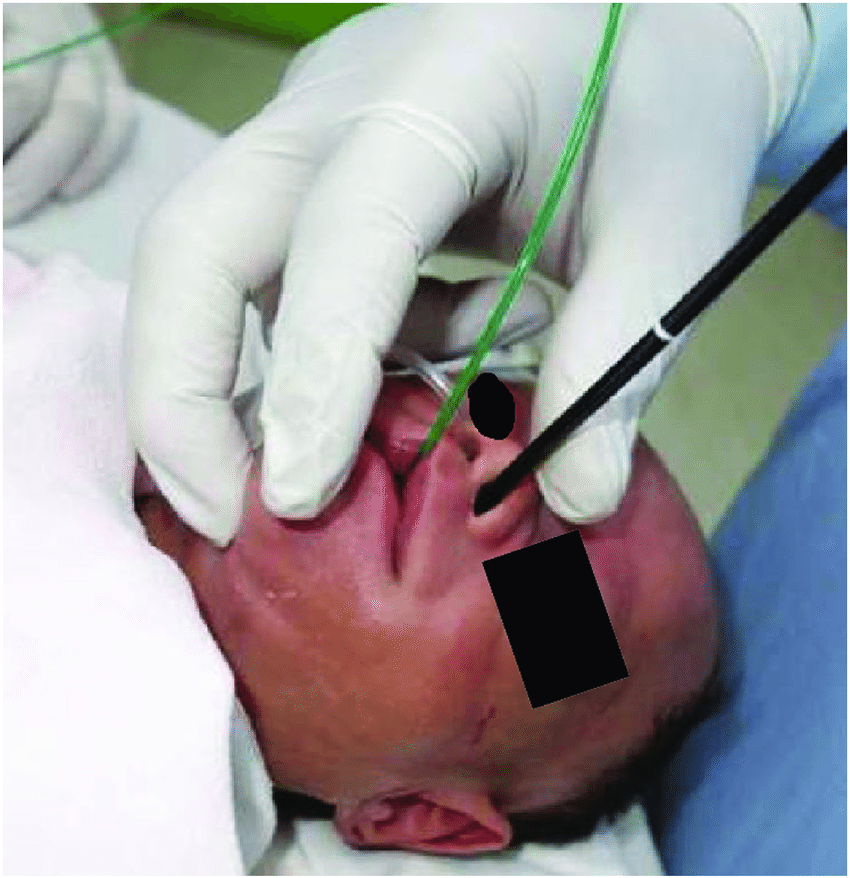
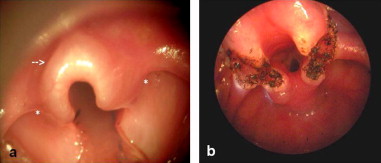
Diagnostic Flexible Nasopharyngolaryngoscopy (FNPLS) is a procedure used to visualize the larynx and assess the structural integrity of the tissues. During the procedure, a flexible scope is inserted through the nose or mouth and passed down into the throat to reach the larynx. This allows the healthcare provider to directly observe the larynx and identify any abnormalities.
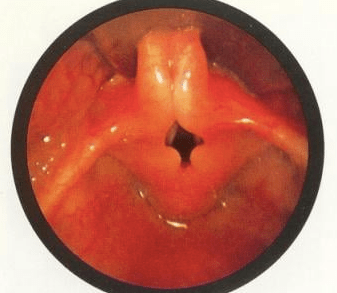
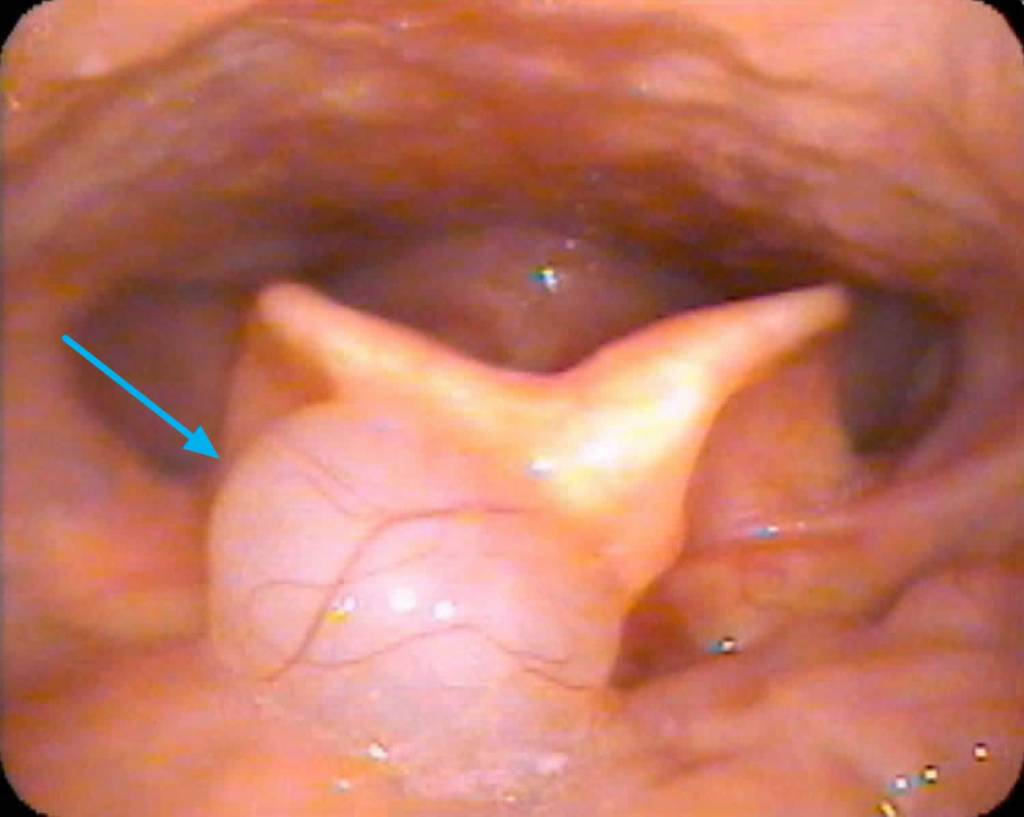
In the case of laryngomalacia, laryngoscopy often reveals specific findings that confirm the diagnosis. The most common finding is the collapse of the supraglottic structures, which include the epiglottis, aryepiglottic folds, and false vocal cords. These structures may appear floppy, redundant, and prolapsed, leading to partial obstruction during breathing. The degree of collapse can vary, ranging from mild to severe.

In addition to assessing the structural aspects, laryngoscopy may also help identify any other associated conditions or anatomical abnormalities (secondary airway lesion/SAL) that could contribute to the symptoms. It allows the healthcare provider to evaluate the movement of the vocal cords, assess the presence of any anatomical obstructions, and determine the overall impact on breathing.
The findings from diagnostic laryngoscopy provide valuable information for guiding the management and treatment plan for laryngomalacia, including the decision for surgical intervention if necessary.
Effective Management Strategies
1. Observation and Reassurance
In mild cases of laryngomalacia, observation and reassurance may be the primary management strategy. Most infants with laryngomalacia outgrow the condition by the age of 18 to 24 months as their laryngeal structures mature. Regular follow-up appointments with the healthcare provider can help monitor the baby’s progress.
2. Positioning Techniques
Simple positioning techniques can help alleviate symptoms and improve breathing for infants with laryngomalacia. Placing the baby in an upright or slightly elevated position during feeding and sleep can reduce the severity of tissue collapse and facilitate better airflow.
3. Dietary Modifications
If gastroesophageal reflux is contributing to the symptoms of laryngomalacia, dietary modifications may be recommended. Feeding the baby in an upright position, smaller and more frequent feedings, and avoiding certain types of food that may trigger reflux can help manage the condition.

4. Medications
In some cases, medications such as acid suppressors or prokinetic agents may be prescribed to reduce the symptoms associated with gastroesophageal reflux. These medications help decrease the acidity of the stomach or promote the movement of food through the digestive system.

5. Surgery
Surgical intervention for laryngomalacia is usually reserved for severe cases that significantly affect the baby’s breathing and overall health (e.g. poor weight gain, failure to thrive). The primary goal of surgery is to alleviate the obstruction and improve the airflow through the larynx. Two commonly performed procedures for laryngomalacia are supraglottoplasty and aryepiglottoplasty.
1. Supraglottoplasty: This surgical procedure involves removing or reshaping the excess floppy tissue in the supraglottic region of the larynx. The surgeon carefully trims and repositions the tissue to open up the airway and reduce collapse during breathing. The specific technique used may vary depending on the individual case and the surgeon’s preference.
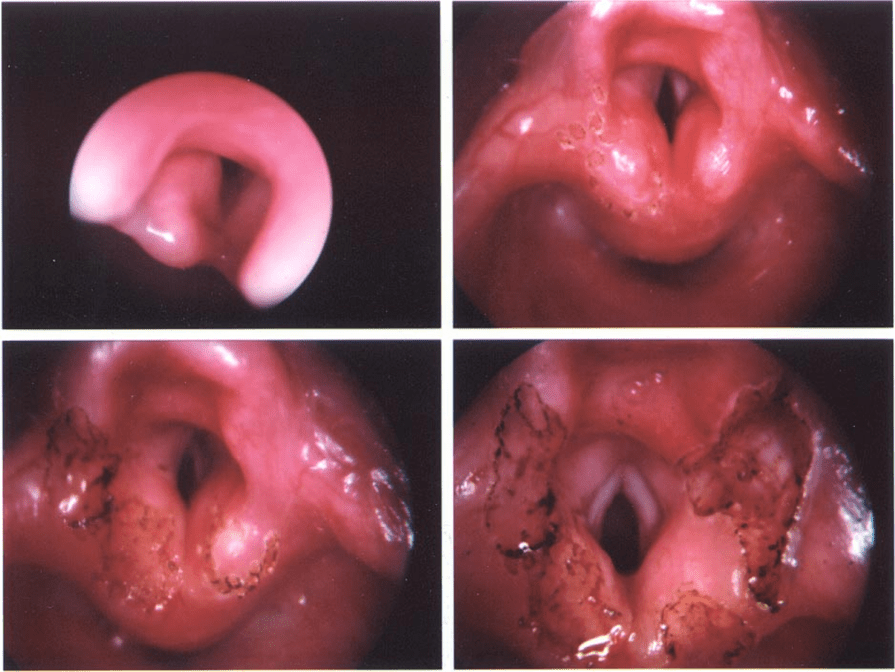
2. Aryepiglottoplasty: This procedure focuses on addressing the collapse of the aryepiglottic folds, which are structures located near the entrance of the larynx. During aryepiglottoplasty, the surgeon makes incisions or removes a portion of the aryepiglottic folds to improve their function and reduce the obstruction.
Surgery for laryngomalacia is typically performed under general anesthesia, and the specific approach depends on the severity of the condition and the individual’s unique anatomical characteristics. The surgical team carefully evaluates the risks and benefits of the procedure before making a decision. The ultimate aim of surgery is to improve the baby’s breathing, reduce symptoms, and enhance overall quality of life.
It is important to note that surgery is not always necessary for laryngomalacia, and many cases can be managed effectively with non-surgical approaches such as observation, positioning techniques, and dietary modifications. The decision for surgery is made on a case-by-case basis, considering the severity of the symptoms, the impact on the baby’s health, and the response to conservative management strategies.
Parental Support and Coping Strategies
Caring for a baby with laryngomalacia can be emotionally challenging for parents. It is essential to seek support from healthcare professionals, join support groups, and connect with other parents who have experienced similar situations. Sharing experiences, gaining knowledge, and receiving emotional support can help parents navigate the journey and cope with the challenges associated with laryngomalacia.

Conclusion
Laryngomalacia is a relatively common condition in infants characterized by the collapse of the laryngeal tissues during breathing. While it can cause concern for parents, it is important to recognize the signs and symptoms and implement effective management strategies. With proper monitoring, reassurance, positioning techniques, dietary modifications, and, in rare cases, surgical intervention, infants with laryngomalacia can thrive and overcome this condition. Seeking support from healthcare professionals and connecting with other parents can provide valuable guidance and emotional support throughout the journey of managing laryngomalacia.






Leave a comment