



















Good morning, everyone. In today’s session, we’ll delve into a challenging case from last year’s edition of The Laryngoscope. It’s about an oroantral fistula, and we’ll explore the surgical approach for managing it.
What is fistula?
A fistula is an abnormal connection between an organ, vessel, or intestine and another organ, vessel or intestine, or the skin. Fistulas can be thought of as tubes connecting internal tubular structures, such as arteries, veins, or intestine, to one another or to the skin.
So what is oroantral fistula? And what causes it?
Oroantral fistula (OAF) is a pathological and epithelialized pathway between the oral cavity and maxillary sinus due to extraction of the upper molars, dental infection, trauma, radiation therapy, osteomyelitis, orthognathic surgery, or dental implants. Upper molars and premolars extraction is considered the most common etiology of OAF.
Oroantral fistulas can cause problems like food or liquid entering the sinus, leading to infection and discomfort. Small fistulas (<5 mm) can heal spontaneously. However, OAF larger than 5 mm or those that have not been resolved within 3 months usually requires surgical treatment.
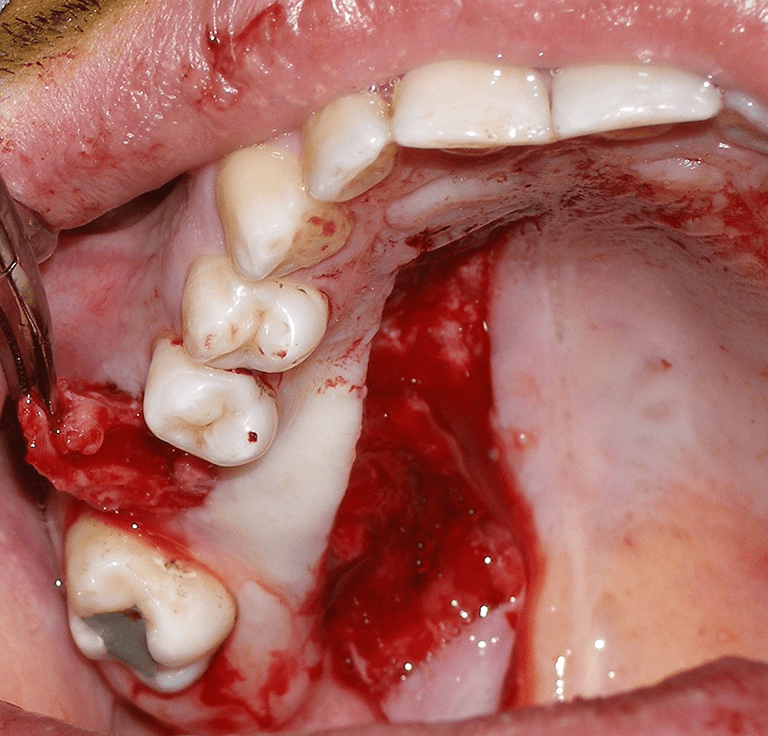
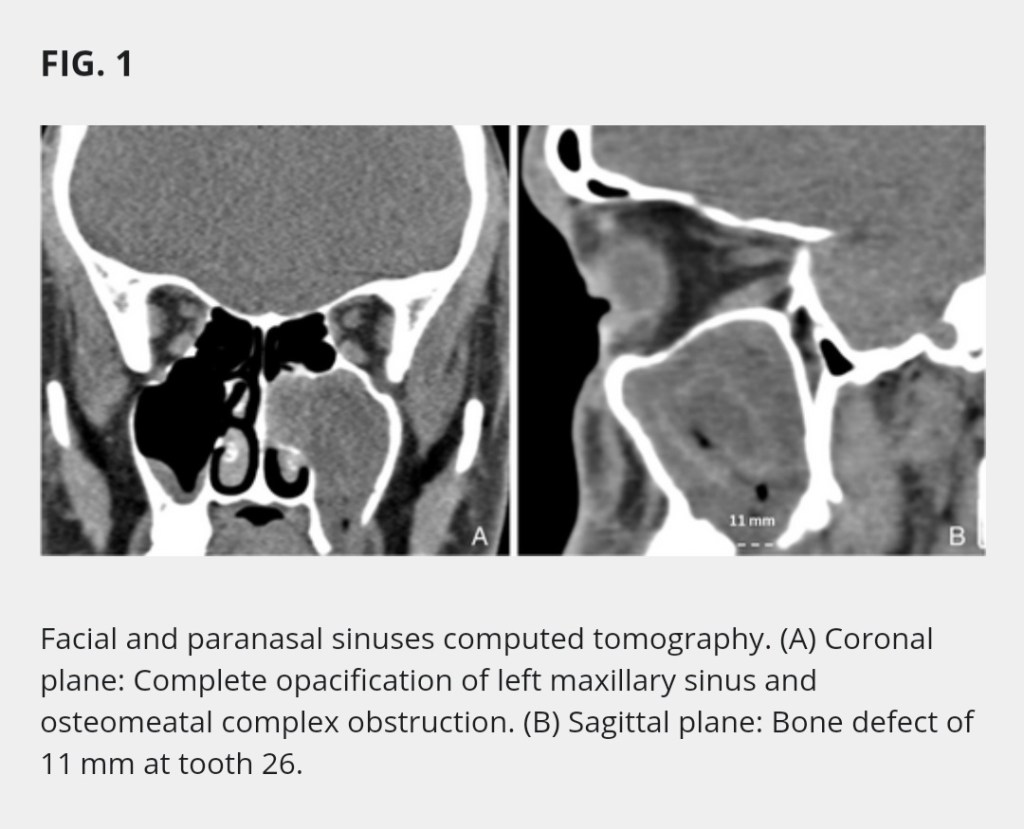
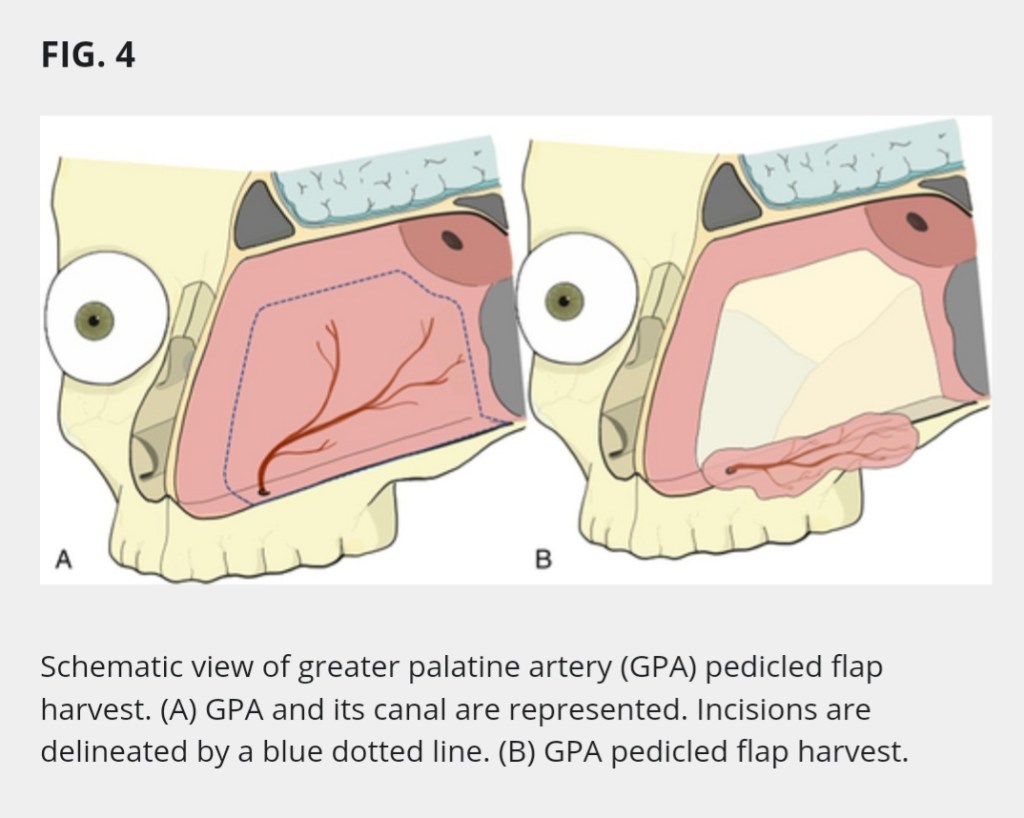
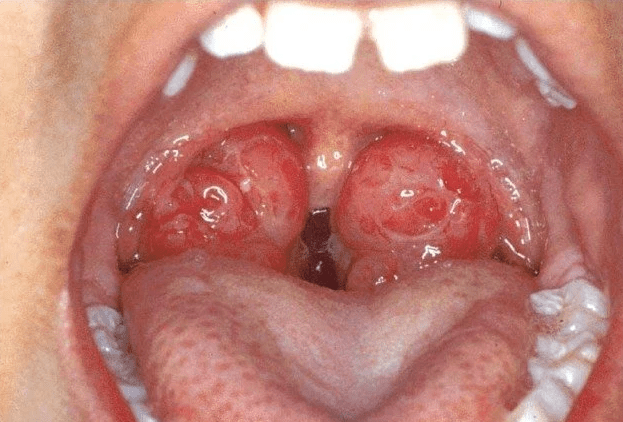
This case – a 30-year-old man visited the emergency department with a history of 4 months of purulent nasal discharge and facial pain in the context of upper left molar extraction that did not respond to long-term antibiotic treatment. Nasal endoscopy showed purulent discharge coming from the left middle meatus and a bulging uncinate process. Oral cavity inspection manifested granulation tissue with purulent discharge at the site of tooth 26. Facial and paranasal sinuses computed tomography (CT) was performed, it showed an 11 mm bone defect at the left maxillary floor concerning tooth 26 and a complete opacification of the maxillary sinus with osteomeatal complex obstruction
Kindly go here to see the full article

Video of the procedure can be downloaded here (162mb)






Leave a comment