




















Chronic Rhinosinusitis: Diagnosis and Investigations
How ENT Specialists in Kuala Lumpur Accurately Identify Sinus Disease
By the time many patients reach my clinic, they’ve already been told they have “sinus” more than once. Some have had multiple courses of antibiotics. Others have tried sprays, antihistamines, even traditional remedies. Yet one key step is often missing:
👉 A proper diagnosis.
Chronic rhinosinusitis (CRS) cannot be accurately diagnosed based on symptoms alone. Modern ENT practice relies on a combination of clinical assessment and targeted investigations to confirm the diagnosis, identify the subtype, and guide treatment.
Let’s walk through how CRS is properly diagnosed — and why guessing is no longer acceptable.
Why Symptoms Alone Are Not Enough
Blocked nose, facial pressure, headache, and post-nasal drip are common complaints. But here’s the catch:
- Not all blocked noses are sinus-related
- Not all facial pain comes from sinuses
- Not all “sinus headaches” are actually sinus disease
This is why evidence-based ENT guidelines emphasise that objective evidence of sinus inflammation is required to diagnose CRS.
Think of it like diagnosing high blood pressure. You wouldn’t rely on how someone feels — you’d measure it.
Step 1: Detailed ENT History (More Important Than You Think)
A thorough consultation sets the foundation.
An ENT specialist will explore:
- Duration of symptoms (especially >12 weeks)
- Nasal blockage pattern (one-sided vs both sides)
- Presence of smell loss
- Response to previous medications
- Allergy history
- Asthma or aspirin sensitivity
- Environmental exposure (important in Kuala Lumpur)
This helps distinguish CRS from:
- Allergic rhinitis alone
- Migraine or tension headache
- Non-sinus facial pain
Step 2: Nasal Endoscopy – The Cornerstone Investigation
If there is one investigation that truly changes management, it’s nasal endoscopy.
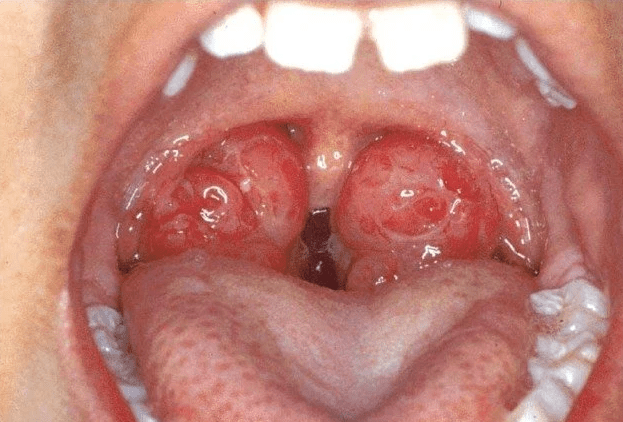
Using a thin camera, an ENT specialist can directly visualise:
- Nasal lining inflammation
- Nasal polyps
- Thick mucus or discharge
- Narrowed sinus drainage pathways
- Structural abnormalities
This procedure is:
- Quick
- Performed in the clinic
- Usually well tolerated
Most importantly, it provides objective evidence of disease — a requirement for diagnosing CRS according to international standards.
For many Kuala Lumpur patients, this is the first time they’ve actually seen what’s causing their symptoms.
Step 3: CT Scan of the Sinuses (When and Why)
A CT scan of the paranasal sinuses is the gold standard imaging for CRS — but it’s not needed for everyone.
It is typically performed when:
- Symptoms persist despite appropriate treatment
- Surgery is being considered
- Anatomy needs detailed assessment
- Complications are suspected
A CT scan shows:
- Sinus opacification
- Mucosal thickening
- Blocked drainage pathways
- Anatomical variations
Important clarification:
👉 Plain sinus X-rays are outdated and unreliable.
Modern ENT practice no longer uses them to diagnose CRS.
Step 4: Allergy Assessment (A Key Piece of the Puzzle)
Because allergic rhinitis is a major contributor to CRS in Malaysia, allergy evaluation is often recommended.
This may include:
- Skin prick testing
- Blood tests for specific IgE
- Correlation with symptom patterns
Identifying allergic triggers allows:
- Targeted allergen avoidance
- Better medical control
- Reduced recurrence of symptoms
Treating CRS without addressing allergy is like drying the floor while the tap is still running.
Step 5: Additional Tests in Selected Patients
In more complex or severe cases, further investigations may be required, such as:
- Blood tests for eosinophilia
- Immune function tests
- Nasal cultures (rarely routine)
- Assessment for asthma or aspirin sensitivity
These are particularly relevant in patients with:
- Severe nasal polyps
- Poor response to standard treatment
- Recurrent disease after surgery
Why Accurate Diagnosis Matters
A precise diagnosis allows the ENT specialist to:
- Classify CRS subtype
- Tailor treatment
- Avoid unnecessary antibiotics
- Decide if surgery is appropriate
- Plan long-term management
CRS is not a “trial-and-error” condition. The better the diagnosis, the better the outcome.








Leave a comment