



















Introduction: Why “Vertigo” Isn’t Just One Condition
“I feel dizzy” is one of the most common and most complex complaints in clinical practice.
But not all dizziness is created equal. What patients describe as “vertigo” may stem from nine very different underlying conditions, each requiring a unique diagnostic and therapeutic approach.
In this evidence-based guide, we break down 9 distinct diagnoses associated with vertigo and imbalance, with clinical insights drawn exclusively from consensus statements and peer-reviewed research in renowned journals like Otology & Neurotology, Journal of Vestibular Research, and Neurology.

1. Post-Concussion Vestibular Dysfunction
🔍 What It Is
Vestibular symptoms following mild traumatic brain injury (mTBI), affecting up to 50% of concussion patients.
🧠 Key Mechanism
Shearing forces disrupt the vestibulo-ocular reflex (VOR), otolithic organs, or central pathways—often alongside visual motion sensitivity or migraine.
🩺 Clinical Clues
- Dizziness starting within 7 days of head injury
- Worsening with screen use, reading, or busy visual environments
- Persistent symptoms >3 months = Post-Concussion Syndrome
💡 Management Takeaway
Vestibular Rehabilitation Therapy (VRT) focusing on gaze stabilization is first-line. Early referral improves outcomes.
📚 Source: Gottshall KR, et al. Vestibular Rehabilitation for Patients with Traumatic Brain Injury. Otology & Neurotology. 2017;38(8):e269-e275.
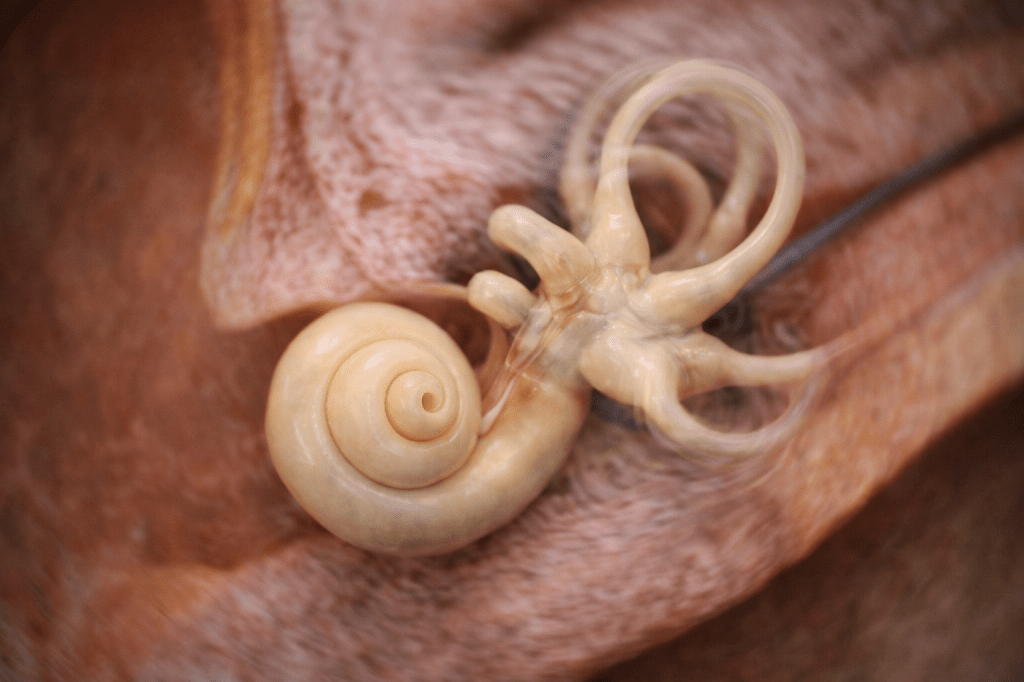
2. Presbyvestibulopathy (PVP): Age-Related Vestibular Decline
🔍 What It Is
A Barany Society-defined syndrome of chronic imbalance in older adults due to age-related vestibular degeneration, without other neurological disease.
🧠 Key Mechanism
Natural loss of vestibular hair cells, nerve fibers, and otoconia → reduced VOR gain and balance reserve.
🩺 Clinical Clues
- Chronic unsteadiness (not acute spinning)
- Worse in darkness or on uneven surfaces
- Mild oscillopsia with quick head turns
💡 Management Takeaway
Focus on fall prevention + balance-specific VRT. Think “vestibular fitness” for aging patients.
📚 Source: Agrawal Y, et al. Presbyvestibulopathy: Diagnostic Criteria Consensus Document. Journal of Vestibular Research. 2019;29(4):161-170.
3. Bilateral Vestibular Loss (BVL)
🔍 What It Is
Significant reduction or absence of vestibular function in both ears, a disabling condition affecting spatial orientation.
🧠 Key Mechanism
Ototoxicity (e.g., gentamicin), autoimmune disease, or meningitis destroy bilateral vestibular input → loss of VOR → retinal slip.
🩺 Clinical Clues
✅ Oscillopsia (world appears to bounce during head movement)
✅ Severe imbalance, especially without visual cues
✅ Positive head impulse test bilaterally
💡 Management Takeaway
Avoid further ototoxicity. Prioritize sensory substitution training via VRT. Vestibular implants remain investigational.
📚 Source: Strupp M, et al. Diagnosis and Management of Bilateral Vestibulopathy. Journal of Neurology. 2017;264(1):1-8.
4. Cervicogenic Dizziness
🔍 What It Is
Dizziness originating from abnormal proprioceptive input from the cervical spine, often after whiplash or with chronic neck pain.
🧠 Key Mechanism
Mismatch between neck proprioception, vision, and vestibular signals → sensory conflict → dizziness.
🩺 Clinical Clues
- Dizziness triggered specifically by neck movement or posture
- Concurrent neck pain/stiffness
- Normal vestibular testing (diagnosis of exclusion)
💡 Management Takeaway
Manual therapy + cervical proprioceptive retraining. Rule out peripheral vestibular causes first.
📚 Source: Treleaven J. Sensorimotor Disturbances in Neck Disorders. The Spine Journal. 2008;8(1):100-108.
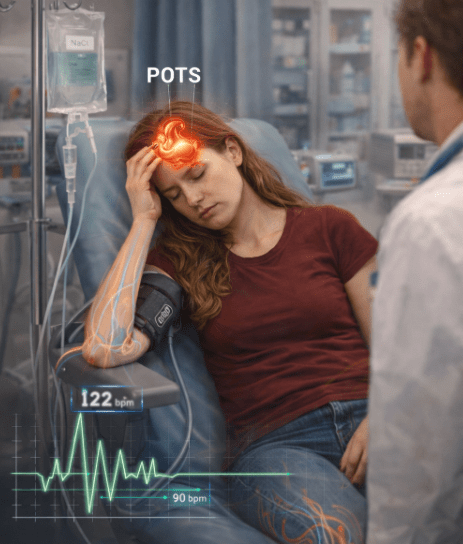
5. Postural Orthostatic Tachycardia Syndrome (POTS)
(Note: Often confused with “POCS”—clarifying the terminology)
🔍 What It Is
A form of dysautonomia where standing triggers excessive heart rate increase → cerebral hypoperfusion → lightheadedness.
🧠 Key Mechanism
Autonomic dysfunction → venous pooling → compensatory tachycardia without adequate BP regulation.
🩺 Clinical Clues
✅ Heart rate ↑ ≥30 bpm within 10 min of standing (adults)
✅ Symptoms improve when lying down
✅ Often accompanied by “brain fog,” fatigue, palpitations
💡 Management Takeaway
Non-pharmacologic first: hydration, salt, compression garments, recumbent exercise. Refer to cardiology/neurology for refractory cases.
📚 Source: Sheldon RS, et al. 2015 HRS Expert Consensus on POTS. Heart Rhythm. 2015;12(11):e41-e63.

6. Mal de Débarquement Syndrome (MdDS)
🔍 What It Is
A persistent sensation of rocking/swaying after disembarking from passive motion (cruise, flight, long drive).
🧠 Key Mechanism
Failure of vestibular adaptation post-motion exposure; emerging evidence points to cortical network hyperconnectivity.
🩺 Clinical Clues
✅ Rocking sensation improves when in passive motion (e.g., driving)
✅ Worse when stationary or stressed
✅ Often triggered by hormonal changes or stress
💡 Management Takeaway
No universal cure. Trial of vestibular rehab, benzodiazepines (short-term), or neuromodulation (rTMS) in specialized centers.
📚 Source: Cha YH. Mal de Debarquement. Frontiers in Neurology. 2020;11:598.

7. Persistent Postural-Perceptual Dizziness (PPPD)
🔍 What It Is
The most common chronic vestibular disorder, a functional brain network disorder triggered by an acute vestibular event.
🧠 Key Mechanism
Maladaptive compensation: over-reliance on vision + heightened threat monitoring → chronic dizziness without structural damage.
🩺 Clinical Clues
✅ Symptoms >3 months
✅ Worsened by: upright posture, motion, complex visual scenes (e.g., grocery stores)
✅ Often follows vestibular neuritis, migraine, or anxiety
💡 Management Takeaway
Multimodal therapy is essential:
🔹 VRT for visual motion desensitization
🔹 SSRI/SNRI to modulate neural gain
🔹 CBT to address symptom-related anxiety
📚 Source: Staab JP, et al. PPPD Diagnostic Criteria: Barany Society Consensus. Journal of Vestibular Research. 2017;27(5-6):201-216.

8. Psychogenic / Anxiety-Related Dizziness
🔍 What It Is
Dizziness primarily driven by panic disorder, generalized anxiety, or somatic symptom disorder, distinct from PPPD but often overlapping.
🧠 Key Mechanism
Hyperventilation → cerebral vasoconstriction; heightened interoceptive awareness → misinterpretation of normal sway.
🩺 Clinical Clues
- Dizziness tied to stress or panic attacks
- Descriptions like “floating,” “detached,” or “spaced out”
- Normal vestibular and neurological exams
💡 Management Takeaway
Treat the underlying anxiety: CBT, breathing retraining, and SSRIs. Avoid reinforcing illness behavior.
📚 Source: Staab JP & Ruckenstein MJ. Psychogenic Dizziness versus Anxiety. Psychosomatic Medicine. 2007;69(7):679-685.

9. Sleep Apnea (OSA) & Dizziness: The Overlooked Link
🔍 What It Is
Obstructive Sleep Apnea is an independent risk factor for chronic dizziness and poor vestibular compensation.
🧠 Key Mechanism
Intermittent nocturnal hypoxia + sleep fragmentation → impaired central vestibular processing + reduced neuroplasticity.
🩺 Clinical Clues
✅ Morning dizziness + excessive daytime sleepiness
✅ Snoring, witnessed apneas, non-restorative sleep
✅ Poor response to standard vestibular therapy
💡 Management Takeaway
Screen for OSA in refractory dizziness. CPAP therapy often improves balance and reduces dizziness severity.
📚 Source: Lin YH, et al. OSA and BPPV Association. The Laryngoscope. 2016;126(5):1239-1243.
🎯 Key Takeaways for Clinicians
1️⃣ Precision matters: “Vertigo” is a symptom, not a diagnosis. Subtype identification guides therapy.
2️⃣ Think multimodal: Many chronic vestibular disorders (PPPD, POTS, MdDS) require combined medical, rehabilitative, and psychological approaches.
3️⃣ Screen broadly: Don’t miss sleep apnea, cervical contributions, or autonomic dysfunction in “refractory” cases.
4️⃣ Cite consensus: Use Barany Society criteria and high-impact journal guidelines to standardize care.
❓ Frequently Asked Questions (FAQ)
Q: Can one patient have more than one of these diagnoses?
A: Absolutely. Comorbidity is common (e.g., PPPD + migraine, BVL + PVP). A layered diagnostic approach is essential.
Q: When should I refer to a vestibular specialist?
A: If symptoms persist >4–6 weeks despite initial management, or if red flags exist (neurological deficits, sudden hearing loss, ataxia).
Q: Are these conditions “all in the patient’s head”?
A: No. Even functional disorders like PPPD involve measurable changes in brain network processing. Validation + targeted therapy yields best outcomes.
🔗 Helpful Resources (External Links)
- Barany Society Diagnostic Criteria
- Vestibular Disorders Association (VeDA)
- American Academy of Otolaryngology – Dizziness Resources
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment of vestibular disorders. Sources cited are from peer-reviewed, high-impact medical journals.
Last Updated: 8/3/26 | Reviewed by: Dr Ameen, ENT Specialist Kuala Lumpur










Leave a comment