Written by Dr Ameen, ENT Specialist Kuala Lumpur
Children can adapt surprisingly well to airway obstruction

Children have a remarkable ability to adapt to partial airway obstruction. Even when the tonsils are enlarged and occupy significant space in the throat, many children continue to breathe by switching from nasal breathing to mouth breathing.
This adaptation allows them to maintain oxygen intake, but it is not a normal or ideal breathing pattern. Because the change happens gradually, parents may not immediately notice it.

Why enlarged tonsils affect airflow

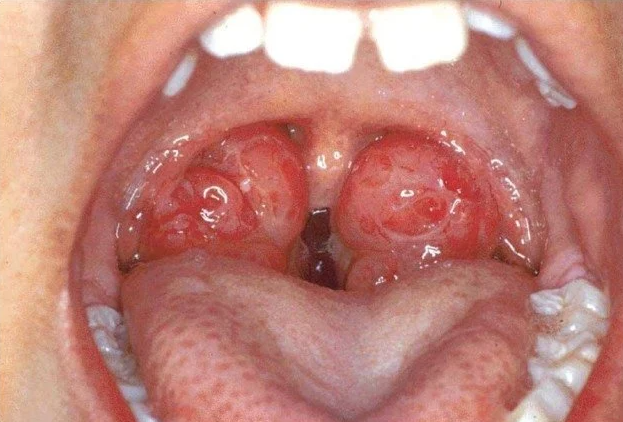
The tonsils are located at the back of the throat. When they become enlarged, they reduce the space available for airflow, especially during sleep when muscle tone naturally decreases.
This narrowing forces the body to find an alternative route for breathing. The mouth becomes the easiest pathway, especially at night.
Mouth breathing is a compensatory mechanism, not a normal habit


Mouth breathing helps bypass the obstruction temporarily. However, it comes with consequences. The nose is designed to filter, humidify, and warm the air before it reaches the lungs. Mouth breathing bypasses these protective functions.
Over time, this can lead to dryness of the throat, increased risk of infections, and poor sleep quality.
Hidden effects on sleep and behaviour

Children who breathe through their mouth often experience disrupted sleep. Even if they appear to sleep through the night, the quality of sleep may be poor due to repeated airway obstruction.
This can result in:
- Daytime sleepiness
- Poor concentration
- Irritability or hyperactivity
- Learning difficulties
Parents may not immediately link these symptoms to breathing problems.
When should parents be concerned

You should consider an ENT evaluation if your child has:
- Loud snoring most nights
- Mouth breathing during sleep
- Pauses in breathing
- Restless sleep or unusual sleeping positions
Early assessment can prevent long-term complications.

Long-term impact if untreated

If left untreated, chronic mouth breathing can affect facial growth and dental alignment. The child may develop a longer facial structure, crowded teeth, and changes in jaw positioning.
These changes occur gradually and may not be noticeable until later childhood. Early intervention can help guide normal growth and development.

Key takeaway
Children may continue to function despite enlarged tonsils by adapting to mouth breathing. However, this is not a harmless habit. It may affect sleep quality, behaviour, and long-term development. Early recognition and proper ENT assessment can prevent complications and improve your child’s overall health and quality of life.
About the Author
Dr Ameen is an Ear, Nose and Throat (ENT) Specialist based in Kuala Lumpur. He holds an MB BCh BAO (Hons) from Ireland and a Master of Otorhinolaryngology from Universiti Kebangsaan Malaysia.
He has undergone extensive training and has served in major tertiary institutions, including Hospital Kuala Lumpur and Hospital Tunku Azizah Women and Children Hospital, where he managed a broad spectrum of ENT conditions in both adults and children, such as ear disorders, sinus disease, throat conditions, and vertigo.
Dr Ameen currently practices at Sunway Medical Centre Velocity and Columbia Hospital Setapak as a sessional ENT Consultant. His clinical approach is centred on precise diagnosis, evidence-based treatment, and clear, patient-focused communication.












Leave a Reply